
Penile Curvature
Correction of congenital penile curvature is strictly surgical. Prof. Shaeer shows you how!
Correction of Isolated Congenital Penile Curvature
Treatment of congenital penile curvature is strictly surgical, if the degree and direction of penile deviation warrants intervention. There is no medical treatment for congenital penile curvature.
Up to the year 2006, congenital penile curvature was almost exclusively corrected by shortening techniques 1 with the consequent loss in length, or grafting techniques with the consequent loss in rigidity. In 2006, Prof. Osama Shaeer developed the first surgical technique to correct congenital penile ventral curvature with neither loss in length, nor erectile dysfunction; Shaeer’s Corporal Rotation. Since 2006, Rotation of the corporal bodies / rotation of the corpora cavernosa was successfully performed for thousands of penile curvature ( chordee ) patients, developed, improved, and reproduced by other world-class experts.
Table of Contents
What is Congenital Penile Curvature?
- Inborn birth defect
- Curved erect penis
- Normally positioned urethral meatus
- Does not progress over time
Congenital penile curvature or chordee is a congenital abnormality where one aspect of the penis overgrows the other, leading to the penis bending towards the shorter side upon erection. This is to be discriminated from hypospadias and epispadias, where there is poor development of the urethra leading to a urethral meatus that is on the upper surface or lower surface of the penis, a whole other entity. This should also be discriminated from acquired penile curvature which develops later in life, mostly due to formation of firm lumps that pull the penis to one side and shorten it; Peyronie’s disease. In congenital penile curvature without hypospadias, the urethral meatus is normally situated, and there are no firm lumps ( Peyronie’s plaques). Yet, the penis is curved when erect. Shaeer’s Corporal Rotation is designed to correct congenital ventral penile curvature.
Why would congenital penile curvature need surgery?
- May affect coital activity in moderate to severe cases
- May affect body image
Moderate degrees of penile curvature will make sex painful to the partner, possiblly resulting in ulceration and infection. Severe penile curvature may prevent sex altogether since the pain will result in vaginismus, where there is involuntary contraction of the pelvic floor muscles of the female partner, making intromission almost impossible.
Mild degrees of penile curvature negatively affect body image resulting in distress in some men.
Which cases require surgery for congenital penile curvature ?
- Ventral penile curvature >30 degrees
- Dorsal penile curvature >40 degrees
- Lateral penile curvature >20 degrees
Surgery required for congenital ventral penile curvature of more than 30 degrees, dorsal penile curvature of more than 40 degrees, lateral penile curvature of 20 degrees or more. Surgery for multi-axial congenital curvature is decided on individual basis. Those are the degrees that warrant surgery since they will affect sexual function. Nevertheless, surgery can be performed for lesser degrees of penile deviation for esthetic reasons. Check the methods of evaluation of penile curvature .
When should surgery for congenital penile curvature be performed ?
Pediatric urologists will perform surgery for congenital penile curvature in the pediatric age, in childhood. Prof.Shaeer has another opinion, where he prefers to postpone surgery for chordee until after puberty is completed, full adulthood. Neither opinion is based on medical evidence.
Read more…
The rational behind repair is childhood is mainly avoiding psychological trauma, where if you perform the surgery before the age of memory recall, the child will not realize he had penile curvature or surgery for it. The rational behind delaying repair until full growth of the adult penis is two fold:
The sutures for repairing congenital curvature of the penis are too thin. They may easily break with erection of the adult penis, resulting in recurrence. The thicker sutures used for penile curvature surgery in adults cannot be used in childhood. The way around this in a child is to not rely on the permanent thin sutures but to rather make small internal incisions and suture them, relying on the permanent healing of the incisions.
When surgery for chordee is performed in childhood, the penis is yet to grow. There is a possibility that the change in dimensions of the growing penis in puberty will aggravate the curvature, again resulting in recurrence.
What are the Surgical Techniques for Correction of Congenital Penile Curvature ?
Surgery for congenital penile curvature falls into two categories: shortening techniques, or length-preserving techniques. A further sub-classification is corporotomy techniques versus non-corporotomy techniques.
To understand how the surgery for penile curvature is performed, we need basic understanding of the anatomy of the penis.
Read More …
The penis has three main structures, three cylinders, that run along the whole length of the shaft: Two corpora cavernosa, and one corpus spongiosum.
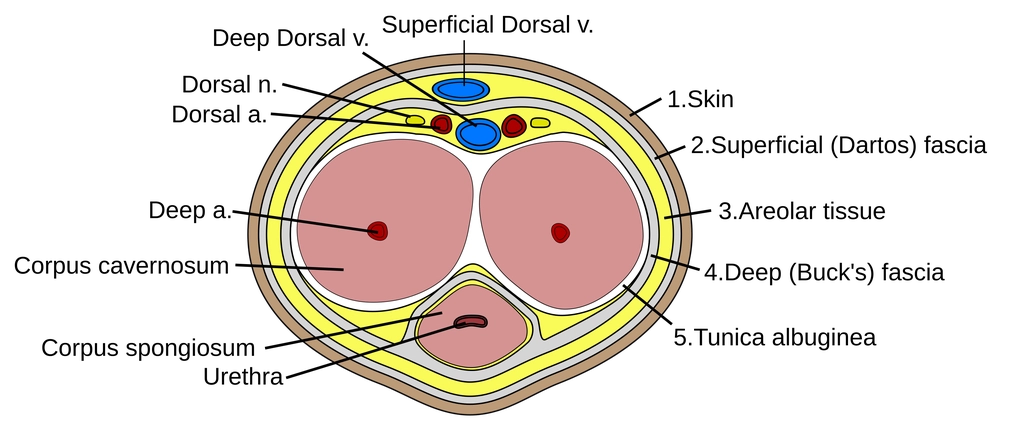
The corpus spongiosum is the one that harbors the urethra, through which urine and semen flow. The corpora cavernosa are the erection cylinders. They fill up with blood for rigid erection to happen. They are responsible for erection. Each corpora cavernosa is a vascular space within a cylinder. In penile curvature cases, the corpora cavernosa have grown disproportionately, with one side longer than the other, leading to a bent penis. The wall of that cylinder is called the Tunica Albuginea. The disproportionate corpora cavernosa are rectified, manipulating them through their walls, the tunica albuginea of each corpus cavernosum, modeling them in the straight shape. This is performed wither by permanent non-absorbable sutures “the non-corporotomy techniques”. Alternatively, repair can be performed by cuts in the tunica albuginea that are sutured together in the modified desired form with absorbable temporary sutures. The cuts heal, maintaining the repair; “the corporotomy techniques”.
Further relevant anatomy is that the two sensory nerves of the penis ( the dorsal nerves of the penis) course on the upper surface of the corpora cavernosa from the base of the penis forwards, next to the two dorsal arteries and the deep dorsal vein. Together they form the neurovascular bundle, that courses in a layer called Buck’s Fascia. The dorsal nerves branch along the way giving sensory supply to the penis. In order to work on the corpora cavernosa without injuring the nerves, the neurovascular bundle has to be set aside: neurovascular bundle mobilization.
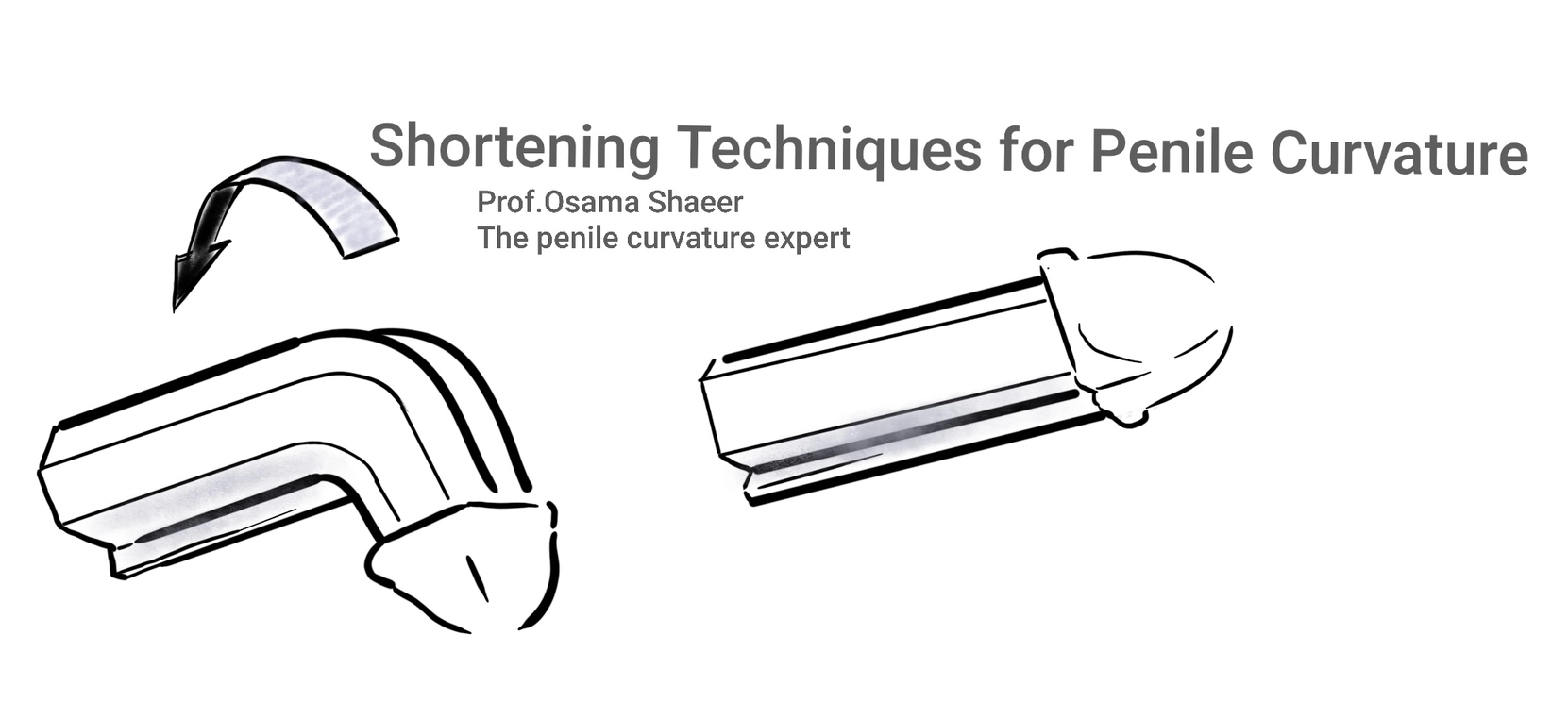
1. Shortening Techniques for Correction of Penile Curvature
- Shortening the convex side to match the concave side
- Simple and cost-effective
- Suitable for penile curvature of any direction
- Will affect length of the penis
Shortening techniques for correction of penile curvature are centered upon shortening the longer convex side of the corpora cavernosa to match the shorter concave side. For example, in a ventral penile curvature pointing downwards, the upper surface (dorsal surface) of the penis is longer, and the lower surface (ventral surface) is shorter. Shortening the dorsal or upper surface will correct the ventral penile curvature. This is on the expense of length of the penis, where the penis will inadvertently become shorter. The greater the degree of curvature, the shorter the penis will be. This is particularly a problem in severe penile curvature, or if the penis is originally short. Hence the advent of Shaeer’s Corporal Rotation which is a length-preserving technique.
Shortening techniques are most suited for milder grades of congenital curvature of the penis, especially when penile length is ample. They are quite simple to perform in mid-level to expert surgeons. They are the original classic way to repair a curved penis.
One of the earliest methods for correction of congenital penile curvature is the Nesbit technique (1965) ref, and its modification; modified Nesbit. The original Nesbit involved an elliptical excision of the tunica albuginea. When the gap edges are sutured back, this shortens the tunica. Modified Nesbit involved cutting vertical incisions and suturing them horizontally, thereby shortening the convex side ref. Both techniques and some subsequent shortening are “corporotomy techniques” where the tunica is opened.
Non-corporotomy techniques were developed later on, where the tunica is shortened without opening it, merely plicating it with permanent non-absorbable sutures. This includes the sixteen dot technique ref, Shaeer’s Double Eight technique ref, Shaeer’s Square Knot technique ref, among others. Non-corporotomy techniques are less invasive, less painful, and with a lower risk for erectile dysfunction.
Shaeer’s Innovations in Shortening Techniques
Shaeer’s Square Knot
This is a shortening technique of the non-corporotomy type that is designed to decrease the possibility of recurrence. Recurrence of penile curvature after surgery is quite rare. With the square knot, the possibility of recurrence is even less. Recurrence is either due to the suture breaking, or due to the suture cutting its way between the longitudinal fibers of the tunica albuginea. As a reminder, the tunica albuginea is the tough covering of the corpora cavernosa, enclosing the erectile tissue. It is composed of longitudinal fibers. Traditional shortening / plication techniques for correction of penile curvature apply sutures along the fibers. With erection, the tight sutures may split the fibers, resulting in recurrence of penile curvature. The square knot distributes the suture entry and exit points along as well as across the longitudinal fibers, thereby decreasing the possibility of recurrence. Furthermore, the knot is inverted inwards towards the tunica rather than outwards towards the skin, thus decreasing the likelihood of the patient feeling the knot.
Shaeer’s Double Eight Technique
The double eight technique is another invention by Prof.Shaeer that aims at decreasing recurrence. The suture entry and exit points are distributed over several non-coinciding points such that the sutures are well-anchored. The double eight technique is originally used in the repair of tears of the tendon Achilles. This is the tendon on the back side of the leg, lower part. It requires the most sturdy repair, otherwise it will tear again. The double eight technique was therefore used in such cases. Prof. Shaeer adopted the double eight technique for correction of penile curvature with minimum recurrence.
Learn more:
2. Length-Preserving Techniques for Correction of Penile Curvature
Length-preserving techniques for correction of congenital penile curvature avoid the decrease in length of the penis that is notorious for shortening techniques. This is particularly important in severe penile curvature and if the penis is originally short. They are most suited for moderate or severe penile deviation, or in mild penile curvature if the patient is concerned about length. Length preserving techniques include incision and grafting, or Shaeer’s Corporal Rotation.
2.a. Incision and Grafting
Incision and grafting was the first no-shortening technique for the curved penis. This involved cutting the concave shorter side open, thereby releasing the tension at the point of maximum curvature and elongating the shorter side. The gap is closed with a graft. However, grafts have a tendency to shrink, thereby resulting in recurrent penile curvature. Furthermore, replacing the tunica albuginea by the weaker graft material compromises the tensile strength of the tunica, possibly resulting in erectile dysfunction.
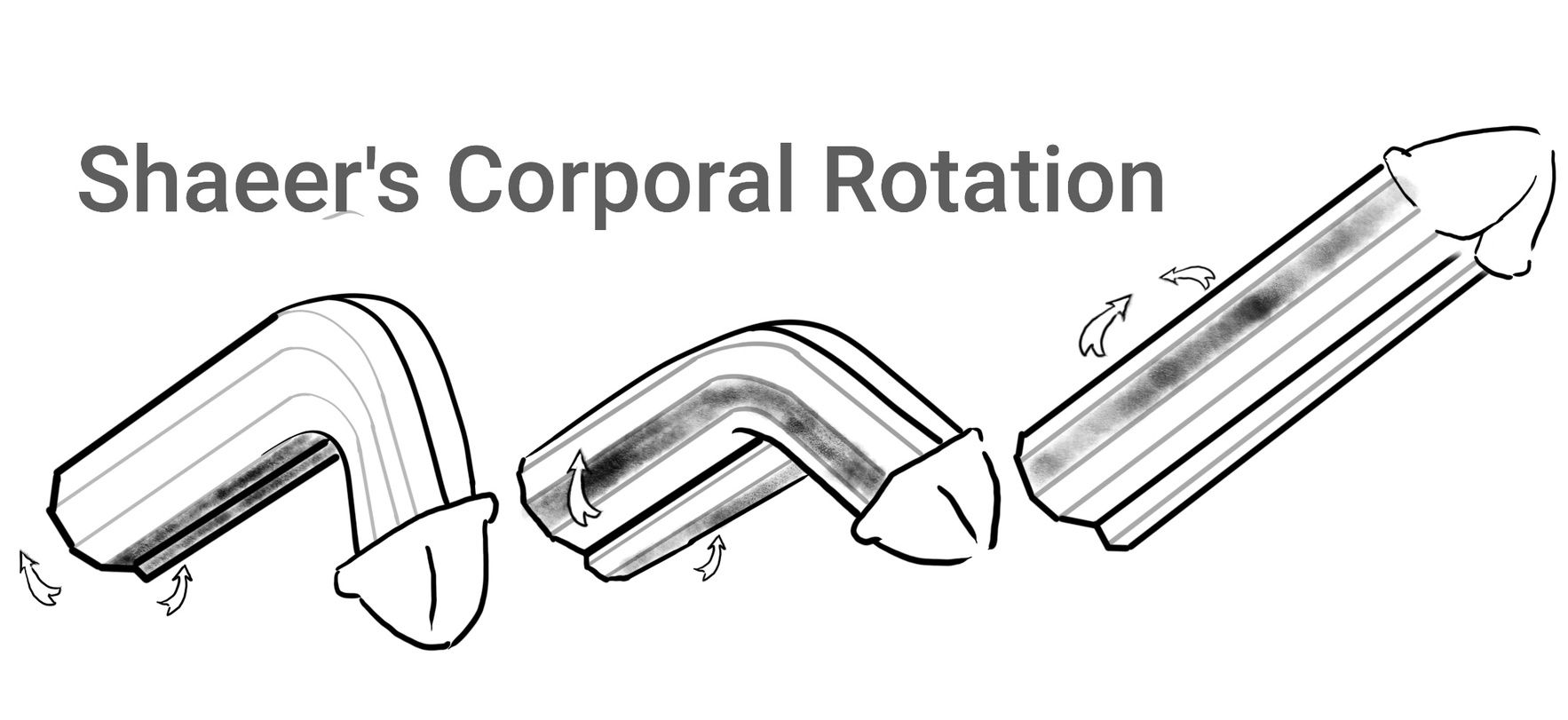
2.b. Shaeer’s Corporal Rotation
Then came Shaeer’s Corporal Rotation. Prof. Osama Shaeer invented corporal rotation in the year 2000, and published the first report thereof in the year 2006. Since then, corporal rotation was followed by some of the most eminent surgeons around the world, and several reports of the positive outcome were published. Prof. Shaeer improved and developed rotation of the corporal bodies further, from Generation I to Generation IV, the latest version : Shaeer’s Corporal Rotation IV.
What is Shaeer’s Corporal Rotation ?
- Corporal rotation is a technique that corrects penile curvature without shortening
- Does not affect erectile function
- Suitable for congenital ventral curvature, possibly dorsal as well.
This is the only surgical technique that can correct any degree of ventral penile curvature of congenital origin, with no or minimal shortening, and without the risk of erectile dysfunction. The basic principle is suturing the upper surface of both corpora cavernosa to one another such that they are rotated inwards 2.
This rotation shifts the shorter ventral surfaces that bend the penis downwards, to the lateral side, right and left, against each other. The downward surface of the right corpus cavernosum is shifted to the right, and that of the left corpus cavernosum is shifted to the left. When the penis is erect, those shifted shorter surfaces are stretched to the max, thereby correcting the curvature with no or minimal shortening. They basically work against each other, neutralizing the pull to the ventral direction.
Advantages of Shaeer’s Corporal Rotation:
- No shortening
- No incision grafting and therefore no erectile dysfunction
- Time-tested technique with many international publications supporting its effectiveness
Disadvantages of Shaeer’s Corporal Rotation:
- Not tested in Peyronie’s disease cases.
- Mild narrowing at the base of the penis
- Only suitable for ventral congenital penile curvature, not lateral.
What is the difference between Shaeer’s Corporal Rotation I, II, III and Shaeer’s Corporal Rotation IV ?
Shaeer’s Corporal Rotation I
The first generation of Shaeer’s Corporal Rotation (Shaeer’s Corporal Rotation I) involved cutting several short incisions on the upper surface of both corpora cavernosa, parallel to each other, and suturing them 3.

Shaeer’s Corporal Rotation II
This was developed further having the incisions be one long incision on the dorsum of each corpus cavernosum. This gave more uniformity to the girth.
Shaeer’s Corporal Rotation III
In SCR III, Prof.Shaeer shifted from corporotomy to non-corporotomy. Instead of cutting incisions and suturing them together, Prof.Shaeer sutured the dorsal surfaces to one another with permanent sutures, without cutting them open; non-corporotomy. This shortening operative time, decreased post-operative pain, and rendered the procedure modifiable in the same session. Meaning that if Prof.Shaeer would like to apply modification to the final shape he could simply remove one stitch and replace it with another, in the same procedure.
Shaeer’s Corporal Rotation III was published in the most prestigious Urology journal; European Urology 4. This was when the world became aware of SCR, and other surgeons started replicating it.

Shaeer’s Corporal Rotation IV
While rotation of the corporal bodies preserves length and rigidity of the penis, its disadvantage was mild narrowing at the proximal half of the penis. This was addressed in Shaeer’s Corporal Rotation IV. Prof.Shaeer noticed that narrowing occurs when correcting the last part of the curvature, the final 20-30 degrees. In Shaeer’s Corporal Rotation IV 2, Prof.Shaeer corrects 70% of the curvature with rotation, and 30% with shortening technique. The end result is full correction, with minimal shortening and minimal narrowing. Shaeer’s Corporal Rotation IV is the latest and most refined version of corporal rotation. Most of Prof.Shaeer’s patients with penile curvature choose Corporal Rotation IV. Yet, a minority will still choose Corporal Rotation III with no shortening technique.
Since he published his first report in 2006, and up to the date of this article in 2006, Prof.Shaeer successfully operated on thousands 1800+ patients from all over the world. Prof. Shaeer operated in three hospitals, his own center of excellence in Cairo Egypt, in Sarajevo Bosnia and Herzegovina, and in Istanbul Türkiye.

Learn more:
Frequently Asked Questions
Does correction of penile curvature result in a shorter penis?
Yes, if performed with the shortening techniques such as 16 dot, Nesbit, or square knot techniques. They are therefore most suited for milder penile curvature degrees with a good length penis. The alternative is the elongation techniques such as Shaeer’s Corporal Rotation most suited for moderate or severe congenital downward curvature
Is surgery for penile curvature urgent? How long can I wait before correcting penile curvature ?
Depends on the cause. If it is a congenital penile curvature, it will not get worse by time. If it is an acquired penile curvature due to Peyronie’s disease, you should wait until it stops progressing before surgical correction.
Can penile curvature recur after surgical correction?
Residual penis curvature is very mild curvature that manifests early after surgery . It does not warrant another surgery. In expert hands, significant recurrence is rare. If it happens, surgery can be repeated. Prof. Shaeer’s techniques help decrease this risk, including the square knot technique and the double eight technique detailed earlier.
When can I have sex after I get my penile curvature corrected?
Some surgeons will permit sex one month after penile curvature surgery. Prof. Shaeer advises three months abstinence before sex to make sure healing is complete and to avoid pain during intercourse
What is the best way to correct penile curvature?
This depends on the cause (congenital penile curvature or acquired penile deviation), direction, degree, erectile function, length of the penis, among other factors. The penile curvature expert factors in all those criteria into the equation to decide on the best way to correct penile deviation. A penile curvature self-test is available online. A penile curvature online consultation or an in-person consultation with an expert is the only way for an accurate evaluation and an informed decision. It can safely be said that elongation techniques are preferred for severe curvatures, with Shaeer Corporal Rotation preferred if the severe curvature is congenital and ventral in direction
How easy is surgery for penile curvature?
In expert hands, penile curvature surgery is a one-day procedure, with the patient able to move freely and leave the hospital on the same day of surgery. Back to office work in one or two days, back to sports in 2-3 weeks.
Is surgery for correction of penile curvature painful?
Not on the long term. Some degree of pain is to be expected after any kind of surgery. If we classify pain as mild moderate or severe, pain after correction of penile curvature is mostly mild to moderate for a few days. After the initial convalescence and recovery, there can be mild pain on erection that may persist for several months. After that, no pain is usually encountered.
Can you feel the sutures used to correct penile curvature ?
If you try to find them you will. It is possible to feel those sutures by hand, felt as a little firm mass under the skin. Nothing harmful, nothing that the partner should feel. Inverting the knots inwards helps concealing them. Using polyester instead of nylon sutures also helps.
Can I do each and every sexual position after correcting my penis curvature?
Yes, but as advised to any man with or without penile curvature, avoid trauma. Sexual trauma can cause major injury in a penis that was never curved. The same applies after correction of penile curvature.
References
- Britton CJ, Jefferson FA 4th, Findlay BL, Sharma V, Hernandez JC, Levine LA, Ziegelmann MJ. Surgical Correction of Adult Congenital Penile Curvature: A Systematic Review. J Sex Med. 2022 Feb;19(2):364-376. doi: 10.1016/j.jsxm.2021.11.017. Epub 2022 Jan 5.mann ↩︎
- Shaeer O, Shaeer K. Shaeer’s corporal rotation IV: length-preserving correction of congenital ventral penile curvature. J Sex Med. 2023 Apr 27;20(5):699-703. doi: 10.1093/jsxmed/qdad028. PMID: 37122108. ↩︎
- Shaeer O. Shaeer’s corporal rotation for length-preserving correction of penile curvature: modifications and 3-year experience. J Sex Med. 2008 Nov;5(11):2716-24. doi: 10.1111/j.1743-6109.2008.00913.x. Epub 2008 Jul 1. PMID: 18624969 ↩︎
- Shaeer O, Shaeer K. Shaeer’s Corporal Rotation III: Shortening-Free Correction of Congenital Penile Curvature-The Noncorporotomy Technique. Eur Urol. 2016 Jan;69(1):129-34. doi: 10.1016/j.eururo.2015.08.004. Epub 2015 Aug 19. PMID: 26298209. ↩︎
- Shaeer O, Shaeer K. Shaeer’s corporal rotation IV: length-preserving correction of congenital ventral penile curvature. J Sex Med. 2023 Apr 27;20(5):699-703. doi: 10.1093/jsxmed/qdad028. PMID: 37122108. ↩︎
Medical Author
Prof. Dr. Osama Shaeer
- Professor of Andrology, Cairo University
- Academician at the European Academy of Andrology
- Seventh President, Middle East Society for Sexual Medicine (MESSM)
- Multiple Awards in Surgical Andrology
- 60+ International Publications
Specialties
- Penile curvature surgery
- Peyronie’s disease
- Penile prosthesis surgery